A really good question came in regarding the choking unconscious protocol. The question was basically this.
A really good question came in regarding the choking unconscious protocol. The question was basically this.
Q: The way the objective is taught regarding choking patients, you progress to chest compressions once the person loses consciousness with or without a pulse. I can understand that and have taught that to my staff BUT those with ACLS certification quickly point out that ACLS still stresses that you do not do chest compressions in a patient with a pulse. I am reviewing my ACLS and I can see the confusion. As I see it, the key is in what you have available to you and in an unconscious choking vs respiratory arrest but I would like to better explain it and to do that I need to make my peace with it too.
Lastly, In response to your training question regarding choking unconscious patient. I know it’s hard to understand some of the changes that take place from time to time with the ILCOR and AHA recommendations.
A: I’ll try and make sense of this particular skill. Once we asses for unconsciousness or lower the unconscious choking patient down to the floor, and after calling 911, we’re going to begin 30 chest compressions immediately and then open the airway, check for obstruction or object in mouth and sweep it out if we see it.
If we don’t see it, we will attempt two breaths, if breaths don’t go in, we will reposition the head tilt and chin lift and try two more breaths(ideally with a one way valve mask in place). If breaths do not go in, we will give 30 more chest compressions and then check mouth for object. Repeat until object is clear, airway is open or help arrives and takes over. If at some point, we sweep an object out and the breath goes in, we then check for a carotid pulse for no more than 10 seconds, if no pulse and no normal breathing…begin CPR. If there is a pulse but patient is not spontaneously breathing, begin rescue breathing at 1 breath every five seconds.
Explanation: The immediate chest compressions are due to a philosophy that the patient was already choking while conscious and instead of assuming that it came out after unconsciousness, we assume that it’s still blocking the airway. The only thing we need to do if not already done, is activate the EMS or 911 system. Then after 30 chest compressions, we check for produced obstruction.
Remember, even in ACLS, we are now less concerned about pulses and more concerned about time from non circulating heart activity or arrest to time of first compression. In other words, if we are not able to detect pulses or are unsure, but the patient is unresponsive and not breathing “normally” (agonal) the science and research is promoting aggressive cardiac compressions and minimization of time between arrest and first compression from CPR. In this scenario, if the choking patient is in cardiac arrest, then they will benefit from receiving 30 chest compressions before we check the airway.
Therefore, in theory, we’ve potentially circulated some residual oxygen to the brain and other vascular organs. If the patient is not in cardiac arrest but simply still choking, the compressions should assist in relieving the obstruction and studies have shown that injury due to non-needed compressions is minimal. This is why the emphasis on aggressive chest compressions.
I hope this helps anyone else who may have had the same question!

 Hello Rescue Fans!
Hello Rescue Fans!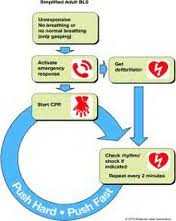 Dear Rescuer,
Dear Rescuer,